

How can we help?
*Indicates a required field.
ADULTS
Limitations:
- One of the coprimary endpoints of this study, change in PPi at 6 months, did not reach statistical significance when comparing the control group to the treatment group. For the total cohort, within-subject changes in both pyridoxal 5’-phosphate (PLP) and PPi were observed after 6 months and over 5 years of treatment
- The control group began treatment 6 months after the treated group, with baseline considered the last assessment before first dose
- During the primary treatment period and in the beginning of the extension phase, the study used lower doses of STRENSIQ than those in the current FDA-approved label
- The open-label extension phase* of the study included 19 adult and adolescent patients. Of the 13 adult patients, 12 had pediatric-onset hypophosphatasia. Three adults were part of the untreated control group during the primary treatment period
- The most common adverse events reported in the adult and adolescent population of Study 4 were injection site reactions1,2
*All data after 6 months are from the open-label extension phase of the study.
324.5 meters
(13,540) at baseline (n=12)5
429.5 meters
(280,696) at 5 years (n=10)5
For adult patients with hypophosphatasia, the minimal clinically important difference (MCID) is estimated at 23 meters and 31 meters based on 2 distribution-based methods.6
{kind=link}
- These results represent adults with pediatric-onset hypophosphatasia with available 6MWT data. Inferences regarding clinical benefit should not be made5
- Reductions in mineralization lag time indicate improved bone mineralization8
- Mineralization lag time was assessed by bone biopsy at baseline and at 1 year in patients receiving STRENSIQ1
- These results reflect data for 6 patients who had values at baseline and 7 patients who had values at 1 year5
6MWT and bone mineralization data are from the open-label extension phase of the study, which included 19 adult and adolescent patients. Of the 13 adult patients, 12 had pediatric-onset hypophosphatasia. Three adults were part of the untreated group during the primary phase. Over the initial duration, the study used lower doses of STRENSIQ than those in the current FDA-approved label.1,2
aEmPATHY: Evaluate and Monitor Physical Performance of Adults Treated with Asfotase Alfa for Hypophosphatasia.10
A similar frequency of adverse events and safety events were reported in EmPATHY as observed in clinical trials. Patients noted reddening and/or tenderness at injection sites with variable intensity and duration sometime during the first 3 months of treatment. No new safety signals emerged from this study.10,11
This small, single-center study may have limited generalizability to a broader adult patient population with hypophosphatasia. This study lacks a comparator arm; however, due to the rare and debilitating nature of hypophosphatasia, the inclusion of an untreated population would be medically unethical and not in line with the descriptive nature of this study. Real-world data collected during routine clinical practice have inherent limitations, such as bias, due to missing data. All patients had a history of ≥1 fracture as part of the enrollment criteria.10,11
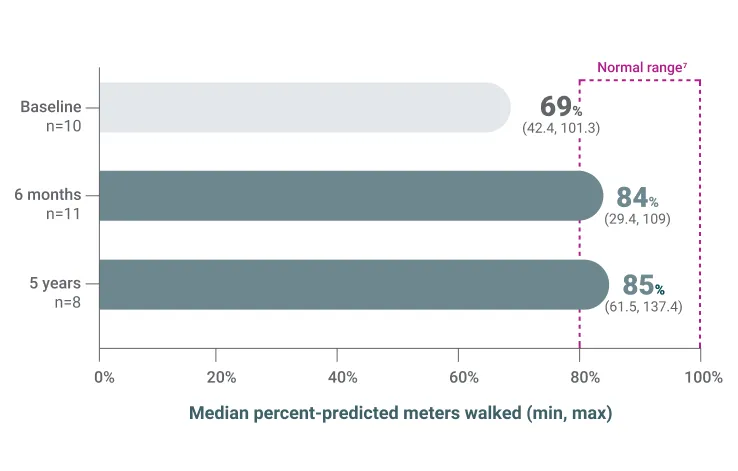
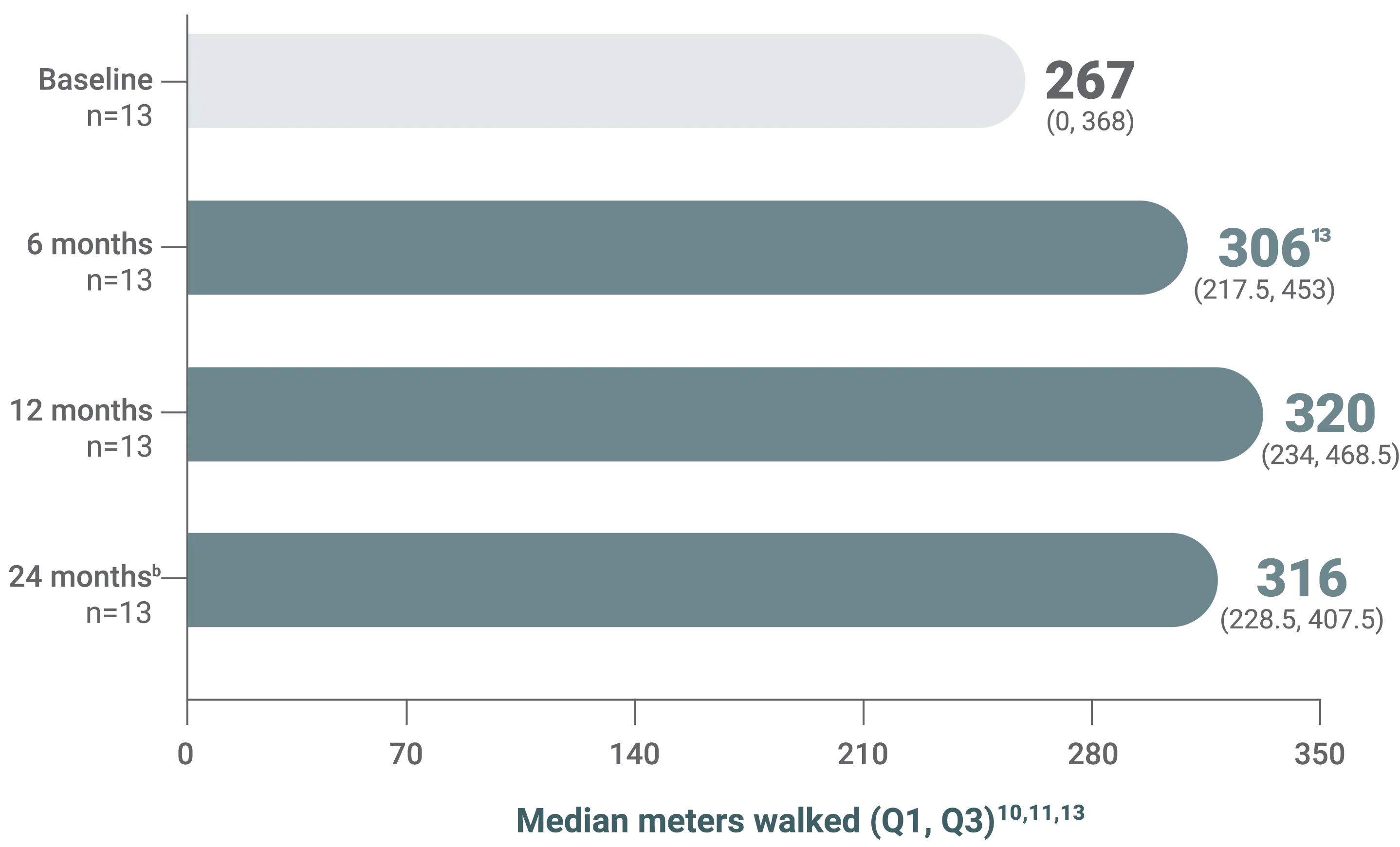
- The minimal clinically important difference (MCID) for hypophosphatasia (~31 meters) from baseline was observed at 6, 12, and 24 months6,10,11
6MWT
Patients walk an indoor, flat, 30-meter walkway with cones at the beginning and end to indicate turns
At the end of 6 minutes, the total distance is recorded.12
At the end of 6 minutes, the total distance is recorded.12
{kind=link}
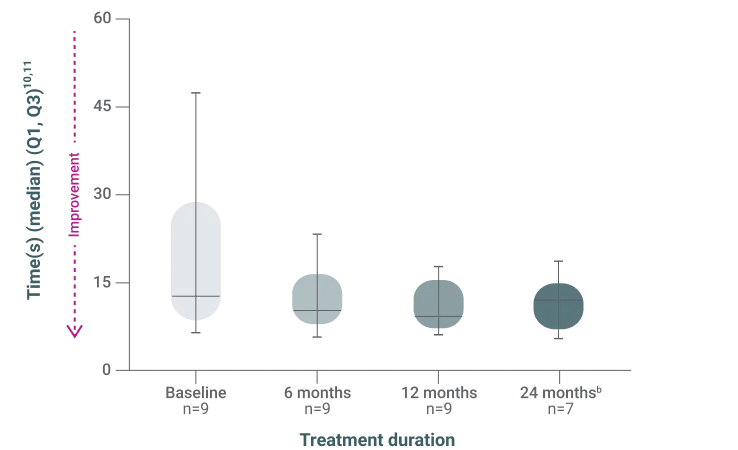
- Differences in median duration time to complete TUG test compared to baseline were observed at 6, 12, and 24 months
TUG test
The time to stand up from a chair, walk to a line 3 meters away, return to the chair, and sit down is recorded
Patients may use assistive devices, if needed.1
Patients may use assistive devices, if needed.1
* TUG test has not been validated in patients with HPP.
{kind=link}
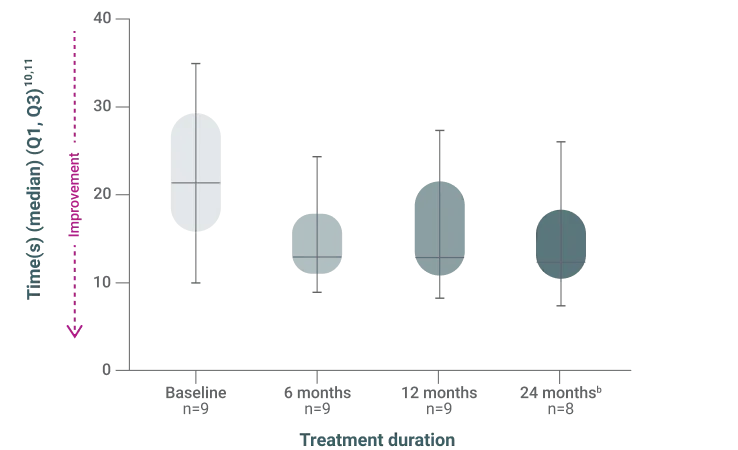
- Differences in median duration time to complete chair rise test compared to baseline were observed at 6, 12, and 24 months
Chair rise test
Measures the time required to complete 5 repetitions of rising from a chair and sitting down
Patients may not use their arms to assist themselves.15
Patients may not use their arms to assist themselves.15
*Chair rise test has not been validated in patients with HPP.
{kind=link}
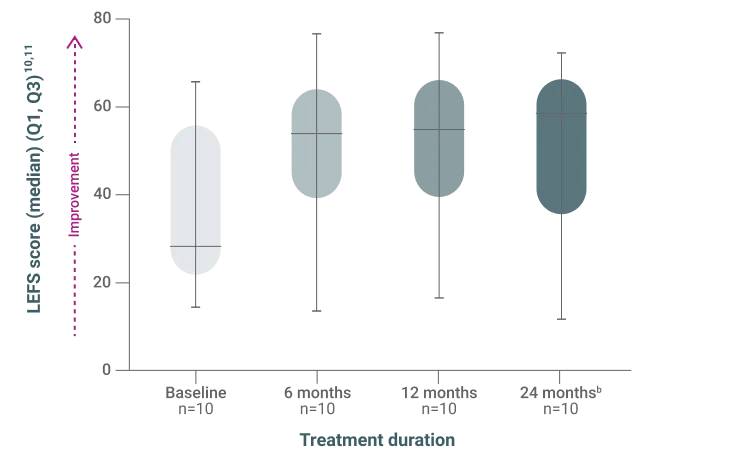
- Differences in median LEFS score compared to baseline were observed at 6, 12, and 24 months
LEFS
A patient-rated outcome measure of lower extremity function in a wide variety of disorders and treatments
Score consists of 20 questions evaluating ability to complete activities with increasing physical demands.16,17
Score consists of 20 questions evaluating ability to complete activities with increasing physical demands.16,17
*LEFS has not been validated in patients with HPP.
{kind=link}
WARNING: HYPERSENSITIVITY REACTIONS INCLUDING ANAPHYLAXIS
Patients treated with enzyme replacement therapies have experienced life-threatening hypersensitivity reactions, including anaphylaxis. Anaphylaxis has occurred during the early course of enzyme replacement therapy and after extended duration of therapy.
Initiate STRENSIQ under the supervision of a healthcare provider with appropriate medical monitoring and support measures. If a severe hypersensitivity reaction (e.g., anaphylaxis) occurs, discontinue STRENSIQ and immediately initiate appropriate medical treatment, including use of epinephrine. Inform patients of the symptoms of life-threatening hypersensitivity reactions, including anaphylaxis and to seek immediate medical care should symptoms occur [see Warnings and Precautions (5.1)].
Initiate STRENSIQ under the supervision of a healthcare provider with appropriate medical monitoring and support measures. If a severe hypersensitivity reaction (e.g., anaphylaxis) occurs, discontinue STRENSIQ and immediately initiate appropriate medical treatment, including use of epinephrine. Inform patients of the symptoms of life-threatening hypersensitivity reactions, including anaphylaxis and to seek immediate medical care should symptoms occur [see Warnings and Precautions (5.1)].
- Life-threatening hypersensitivity reactions, including anaphylaxis, have been reported in STRENSIQ-treated patients. Signs and symptoms consistent with anaphylaxis included difficulty breathing, choking sensation, nausea, periorbital edema, and dizziness. These reactions have occurred within minutes after subcutaneous administration of STRENSIQ and have been observed more than 1 year after treatment initiation. Other hypersensitivity reactions have also been reported in STRENSIQ-treated patients, including vomiting, fever, headache, flushing, irritability, chills, erythema, rash, pruritus, and oral hypoesthesia. Consider the risks and benefits of re-administering STRENSIQ following a severe reaction. If the decision is made to re-administer, monitor patients for a reoccurrence of signs and symptoms of a severe hypersensitivity reaction.
- Lipodystrophy: Localized lipodystrophy, including lipoatrophy and lipohypertrophy has been reported at injection sites after several months in patients treated with STRENSIQ in clinical trials. Advise patients to follow proper injection technique and to rotate injection sites.
- Ectopic Calcifications: Patients with HPP are at increased risk for developing ectopic calcifications. Events of ectopic calcification, including ophthalmic (conjunctival and corneal) and renal (nephrocalcinosis, nephrolithiasis), have been reported in the clinical trial experience with STRENSIQ. There was insufficient information to determine whether the reported events were consistent with the disease or due to STRENSIQ. No visual changes or changes in renal function were reported resulting from the occurrence of ectopic calcifications.
Ophthalmology examinations and renal ultrasounds are recommended at baseline and periodically during treatment with STRENSIQ to monitor for signs and symptoms of ophthalmic and renal ectopic calcifications and for changes in vision or renal function. - Possible Immune-Mediated Clinical Effects: In clinical trials, most STRENSIQ-treated patients developed anti-asfotase alfa antibodies and neutralizing antibodies which resulted in reduced systemic exposure of asfotase alfa. In postmarketing reports, some STRENSIQ-treated patients with initial therapeutic response subsequently developed recurrence and worsening in disease-associated laboratory and radiographic biomarkers (some in association with neutralizing antibodies) suggesting possible immune-mediated effects on STRENSIQ’s pharmacologic action resulting in disease progression. The effect of anti-asfotase alfa antibody formation on the long-term efficacy of STRENSIQ is unknown. There are no marketed anti-asfotase alfa antibody tests. If patients experience progression of HPP symptoms or worsening of disease-associated laboratory and imaging biomarkers after a period of initial therapeutic response to STRENSIQ, consider obtaining anti-asfotase alfa antibody testing by contacting STRENSIQ Medical Information at Alexion at 1-888-765-4747 or by email at medinfo@alexion.com. Close clinical follow up is recommended.
In clinical trials, the most common adverse reactions (≥ 10%) reported were injection site reactions (63%), lipodystrophy (28%), ectopic calcifications (14%), and hypersensitivity reactions (12%). Possible immune-mediated clinical effects have been identified during post-approval use of STRENSIQ.
Drug Interference with Laboratory Tests:
- Laboratory tests utilizing alkaline phosphatase (ALP) as a detection reagent could result in erroneous test results for patients receiving treatment due to the presence of asfotase alfa in clinical laboratory samples. Inform laboratory personnel that the patient is being treated with STRENSIQ and discuss use of an alternative testing platform which does not utilize an ALP-conjugated test system.
- Elevated serum ALP measurements detected through clinical laboratory testing are expected in patients receiving STRENSIQ due to circulating concentrations of asfotase alfa. Do not rely on serum ALP measurements for clinical decision making in patients treated with STRENSIQ.
- Pregnancy & Lactation: There are no available data on STRENSIQ use in pregnant women, the presence of STRENSIQ in human milk, or the effects on the breastfed infant or on milk production, to inform a drug associated risk.
STRENSIQ® (asfotase alfa) is indicated for the treatment of patients with perinatal/infantile- and juvenile-onset hypophosphatasia (HPP).
Please see full Prescribing Information for STRENSIQ (asfotase alfa), including Boxed WARNING regarding hypersensitivity reactions including anaphylaxis.