

strength and mobility1 IN ADOLESCENTS WITH HYPOPHOSPHATASIA
How can we help?
*Indicates a required field.
ADOLESCENTS
AFTER 6 MONTHS1
67% (6/9)
of patients experienced complete or substantial healing of hypophosphatasia-related rickets as measured by the Radiographic Global Impression of Change (RGI-C)*
AFTER 7 YEARS1
100% (9/9)
responder rate
responder rate
Efficacy results reflect data for 9 individuals who reached adolescence (aged 13 to 17 years) during the course of the study.1
*The RGI-C scale quantifies change over time in mineralization and bone structure.2
After 5 years of STRENSIQ treatment, patient had an RGI-C score of +2.67.
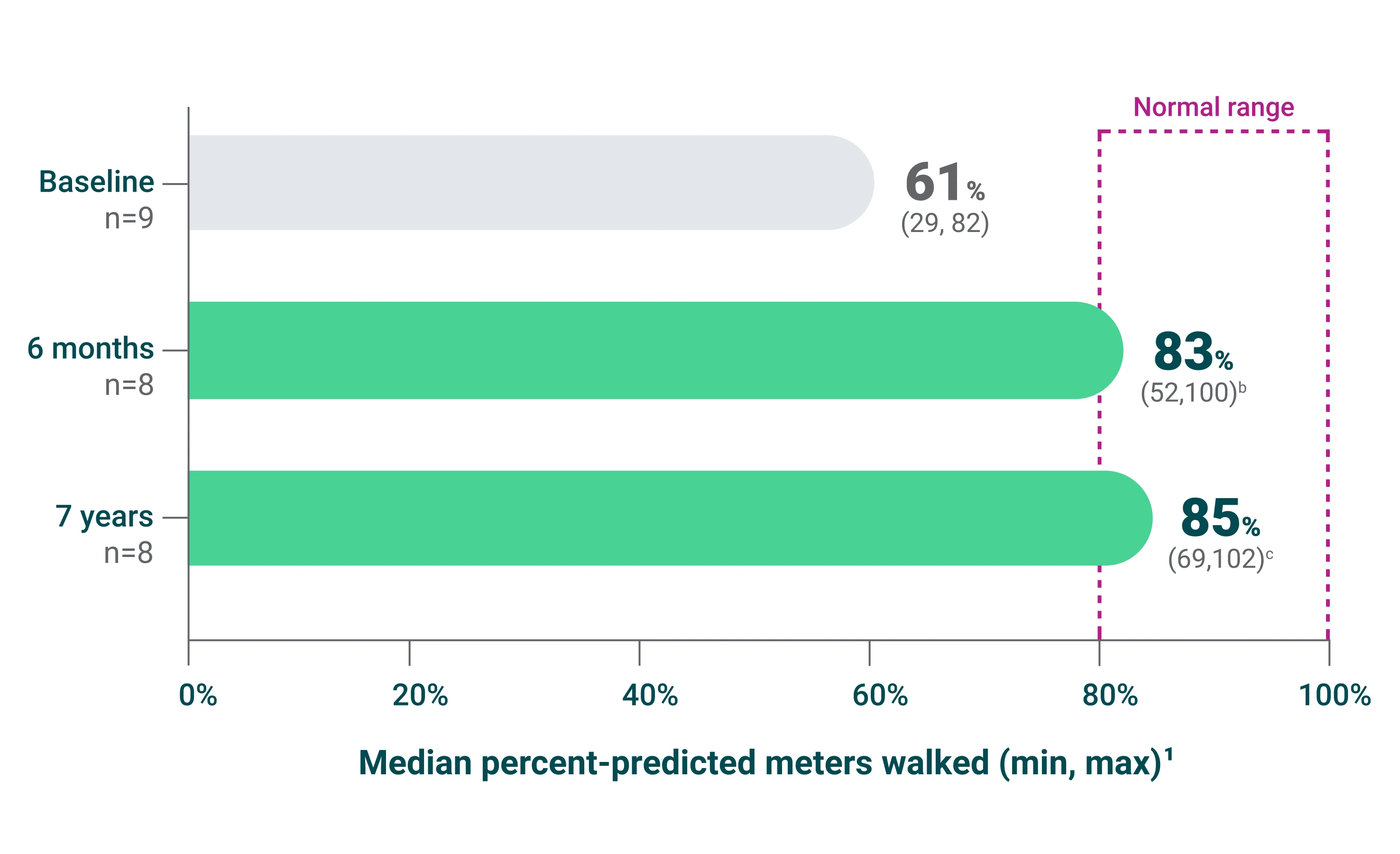
142 meters
median change from baseline in distance walked (511 meters vs 350 meters) (P =0.0078)
AT 7 YEARS1
270 meters
median change from baseline in distance walked (593 meters vs 350 meters) (P =0.0010)
For adolescent patients with hypophosphatasia, the minimal clinically important difference (MCID) is estimated at 33 meters and 43 meters based on 2 distribution-based methods.3
{kind=link}
†Adults with pediatric-onset hypophosphatasia.
WARNING: HYPERSENSITIVITY REACTIONS INCLUDING ANAPHYLAXIS
Patients treated with enzyme replacement therapies have experienced life-threatening hypersensitivity reactions, including anaphylaxis. Anaphylaxis has occurred during the early course of enzyme replacement therapy and after extended duration of therapy.
Initiate STRENSIQ under the supervision of a healthcare provider with appropriate medical monitoring and support measures. If a severe hypersensitivity reaction (e.g., anaphylaxis) occurs, discontinue STRENSIQ and immediately initiate appropriate medical treatment, including use of epinephrine. Inform patients of the symptoms of life-threatening hypersensitivity reactions, including anaphylaxis and to seek immediate medical care should symptoms occur [see Warnings and Precautions (5.1)].
Initiate STRENSIQ under the supervision of a healthcare provider with appropriate medical monitoring and support measures. If a severe hypersensitivity reaction (e.g., anaphylaxis) occurs, discontinue STRENSIQ and immediately initiate appropriate medical treatment, including use of epinephrine. Inform patients of the symptoms of life-threatening hypersensitivity reactions, including anaphylaxis and to seek immediate medical care should symptoms occur [see Warnings and Precautions (5.1)].
- Life-threatening hypersensitivity reactions, including anaphylaxis, have been reported in STRENSIQ-treated patients. Signs and symptoms consistent with anaphylaxis included difficulty breathing, choking sensation, nausea, periorbital edema, and dizziness. These reactions have occurred within minutes after subcutaneous administration of STRENSIQ and have been observed more than 1 year after treatment initiation. Other hypersensitivity reactions have also been reported in STRENSIQ-treated patients, including vomiting, fever, headache, flushing, irritability, chills, erythema, rash, pruritus, and oral hypoesthesia. Consider the risks and benefits of re-administering STRENSIQ following a severe reaction. If the decision is made to re-administer, monitor patients for a reoccurrence of signs and symptoms of a severe hypersensitivity reaction.
- Lipodystrophy: Localized lipodystrophy, including lipoatrophy and lipohypertrophy has been reported at injection sites after several months in patients treated with STRENSIQ in clinical trials. Advise patients to follow proper injection technique and to rotate injection sites.
- Ectopic Calcifications: Patients with HPP are at increased risk for developing ectopic calcifications. Events of ectopic calcification, including ophthalmic (conjunctival and corneal) and renal (nephrocalcinosis, nephrolithiasis), have been reported in the clinical trial experience with STRENSIQ. There was insufficient information to determine whether the reported events were consistent with the disease or due to STRENSIQ. No visual changes or changes in renal function were reported resulting from the occurrence of ectopic calcifications.
Ophthalmology examinations and renal ultrasounds are recommended at baseline and periodically during treatment with STRENSIQ to monitor for signs and symptoms of ophthalmic and renal ectopic calcifications and for changes in vision or renal function. - Possible Immune-Mediated Clinical Effects: In clinical trials, most STRENSIQ-treated patients developed anti-asfotase alfa antibodies and neutralizing antibodies which resulted in reduced systemic exposure of asfotase alfa. In postmarketing reports, some STRENSIQ-treated patients with initial therapeutic response subsequently developed recurrence and worsening in disease-associated laboratory and radiographic biomarkers (some in association with neutralizing antibodies) suggesting possible immune-mediated effects on STRENSIQ’s pharmacologic action resulting in disease progression. The effect of anti-asfotase alfa antibody formation on the long-term efficacy of STRENSIQ is unknown. There are no marketed anti-asfotase alfa antibody tests. If patients experience progression of HPP symptoms or worsening of disease-associated laboratory and imaging biomarkers after a period of initial therapeutic response to STRENSIQ, consider obtaining anti-asfotase alfa antibody testing by contacting STRENSIQ Medical Information at Alexion at 1-888-765-4747 or by email at medinfo@alexion.com. Close clinical follow up is recommended.
In clinical trials, the most common adverse reactions (≥ 10%) reported were injection site reactions (63%), lipodystrophy (28%), ectopic calcifications (14%), and hypersensitivity reactions (12%). Possible immune-mediated clinical effects have been identified during post-approval use of STRENSIQ.
Drug Interference with Laboratory Tests:
- Laboratory tests utilizing alkaline phosphatase (ALP) as a detection reagent could result in erroneous test results for patients receiving treatment due to the presence of asfotase alfa in clinical laboratory samples. Inform laboratory personnel that the patient is being treated with STRENSIQ and discuss use of an alternative testing platform which does not utilize an ALP-conjugated test system.
- Elevated serum ALP measurements detected through clinical laboratory testing are expected in patients receiving STRENSIQ due to circulating concentrations of asfotase alfa. Do not rely on serum ALP measurements for clinical decision making in patients treated with STRENSIQ.
- Pregnancy & Lactation: There are no available data on STRENSIQ use in pregnant women, the presence of STRENSIQ in human milk, or the effects on the breastfed infant or on milk production, to inform a drug associated risk.
STRENSIQ® (asfotase alfa) is indicated for the treatment of patients with perinatal/infantile- and juvenile-onset hypophosphatasia (HPP).
Please see full Prescribing Information for STRENSIQ (asfotase alfa), including Boxed WARNING regarding hypersensitivity reactions including anaphylaxis.